



















Kidney gene implicated in increased heart failure risk
Scientists have identified the first DNA sequence variant common in the population that is not only associated with an increased risk of heart failure, but appears to play a role in causing it.
The variant, a change in a single letter of the DNA sequence, impairs channels that control kidney function.
"It's not a heart gene," says Gerald W. Dorn II, MD, the Philip and Sima K. Needleman Professor of Medicine at Washington University School of Medicine in St. Louis and a lead investigator on the study. "It's a kidney gene. This protein is not even expressed in the heart. Nobody has previously considered that kidney-specific gene defects might predispose you to heart failure."
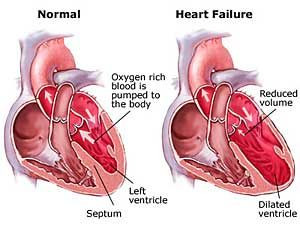
Heart failure is diagnosed when the heart can no longer provide sufficient blood to the body. It can have a number of causes, including high blood pressure, cancer therapy, viral infections of the heart or heart attack.
"It's a syndrome," Dorn says. "You've had sufficient damage to your heart that it doesn't work very well. You collect fluid in your lungs, you swell up, and you have trouble breathing."
The unexpected results highlight the advantage of performing genome-wide studies to find DNA sequence variants associated with disease.
"I was surprised by the finding," says Thomas P. Cappola, MD, assistant professor of medicine at the University of Pennsylvania School of Medicine, also a lead investigator on the study. "This is a good example of how taking unbiased approaches to study human disease can lead you to unexpected targets."
The study, a collaboration between Washington University School of Medicine, the University of Pennsylvania and other institutions, appears Jan. 17 in The Proceedings of the National Academy of Sciences.
In previous work, Dorn and colleagues used a partial genome-wide search technique to define the region of DNA in which sequence changes were associated with heart failure. But most of these sequence changes did not code for a change in protein and appeared not to have actually caused the increased risk. Instead, they served as markers, providing clues that this portion of the genome was worth a closer look.
"We said we've got the right ZIP code, but we're not on the right block," Dorn says.
So Dorn and his team sequenced the neighboring gene, looking for variations in parts of the DNA sequence that do code for proteins.
Studying three groups of Caucasian patients with heart failure, they found one DNA sequence variant that was common in all the groups and was actively involved in making an important protein for the body. A single change in the DNA sequence of a gene called CLCNKA leads to a change from arginine to glycine in the 83rd amino acid of the protein. This protein makes up part of a kidney channel responsible for controlling the secretion of chloride ions into the urine, an important process in maintaining the proper balance of salt and water in the body.
That single amino acid change reduced the channel's ability to shuttle chloride ions across the cell membrane by about half. Dorn hypothesizes that a result of this reduction could be elevated levels of a hormone called renin in the blood. Renin is produced in the kidney and is the first signal in a cascade that can damage the heart. This opens the possibility of helping people who have the variant reduce their risk of heart failure with drugs commonly used to treat high blood pressure, including ACE-inhibitors and aldosterone blockers.
To determine the effectiveness of this approach, Dorn and his colleagues have designed a clinical trial to be performed at Washington University and the University of Pennsylvania that will test whether effects of the risk gene can be opposed by an aldosterone blocker. If so, these findings open the door to tailored individual preventative therapy based on personal genotype, or "personalized medicine."
Over a lifetime, the average person has a one in five chance of developing heart failure. For individuals with one copy of the variant sequence, that risk may increase about 27 percent. For those who have two copies of the variant gene sequence, one from each parent, the risk of developing heart failure increases an estimated 54 percent. About one quarter of all Caucasians have two copies of the variant.
Dorn points out that having one or even two copies of this variant does not, in itself, cause heart failure.
"There are lots of people walking around with this variant who don't have heart failure," Dorn says. "But we think if you have this predisposition and something else happens to you, such as developing high blood pressure or having a small heart attack, that increases your odds of developing heart failure."







